LYTIC BONE LESION
By Dr. KM Liau

When you see lytic bone lesion think of FOGMACHINE.
Most of the lytic lesions are benign conditions with the exception of 'M' (Metastasis and Multiple Myeloma)
SOLITARY LYTIC BONE LESION
Differential Diagnosis (Mnemonic = FOGMACHINES)
F = Fibrous Dysplasia
O = Osteoblastoma
G = Giant Cell Tumour
M = Metastasis / Myeloma
A = Aneurysmal Bone Cyst
C = Chondroblastoma
H = Hyperparathyroidism(brown tumours)/ Hemangioma
I = Infection
N = Non-ossifying Fibroma
E = Eosinophilic Granuloma / Enchondroma
S = Solitary Bone Cyst
FIBROUS DYSPLASIA
Etiology unknown
Most common between 3-15 years of age.
Deformity of long bone (Most common deformity is varus of the proximal femur-"Shepherd's crook deformity") and bone pain.

Shepherd's crook deformity
Fundamental Abnormality Of Fibrous Dysplasia
The fundamental abnormality is replacement of medullary bone by fibrous tissue.
Characteristic X-ray findings:
1. Endosteal scalloping
2. Cortical thinning
3. Homogenous ground-glass appearance
4. Angular deformity at the level of the lesion.

Fibrous Dysplasia
McCune Albright's Syndrome
1 Polyostotic
2. Sexual precocity
3. Cafe-au-lait spots (Coast of Maine)
4. Almost always in a female

Coast of Maine cafe au-lait spot - The lesion has a rough, irregular border

AP view of the left hand demonstrates multiple large expansile "bubbly" lytic lesions
FIBROUS DYSPLASIA - TREATMENT
1. Observation -Prevention of deformity and fracture.
2. Pathologic fracture managed by standard methods according to the site of fracture. Suboptimal alignment will not remodel with time and should not be tolerated.
Surgical treatment principles:
1. Recurrent fracture require internal fixation with intramedullary rods and bone graft.
2. Severe angular deformities- treated with closing wedge osteotomies, bone grafting, and internal fixation.
3. Leg length discrepancy- treated with epiphysiodesis of contralateral limb at the appropriate age.

Fibrous dysplasia of both femur treated with internal fixation
Fibrous Dysplasia Link List
- Fibrous Dysplasia
- Learn more about fibrous dysplasia
OSTEOBLASTOMA
 Osteoblastoma is a solitary, benign and self-limited tumour that produces osteoid and bone. (Large form of osteoid osteoma; >2cm)
Osteoblastoma is a solitary, benign and self-limited tumour that produces osteoid and bone. (Large form of osteoid osteoma; >2cm)Occurs in the posterior element of spine, the metaphysis or diaphysis of long bones, and rarely in the pelvis.
Characteristic X-ray findings of Osteoblastoma
1. Radio-lucent defect with a central density due to ossification.
2. The lesion is well circumscribed and may have a surrounding sclerosis.

Osteoblastoma of proximal humerus
GIANT CELL TUMOUR
 Aetiology unknown)
Aetiology unknown)(Probably arise from zone of osteoclastic activity in skeletally immature patients).
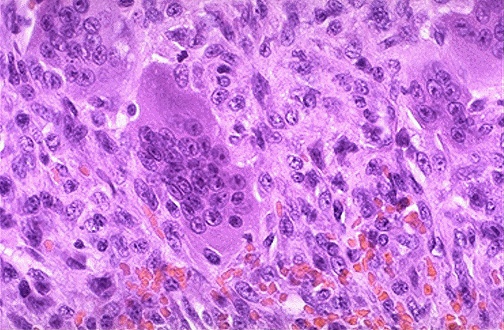
Histology:
Multinucleated osteoclastic giant cells intermixed throughout a spindle cell stroma
Characteristic X-Ray finding of Giant Cell Tumour
1. Solitary expansile lytic lesion
2. Location: Metaphyseal and Juxta-articular (adjacent to joint)
3. Multiple septation (soap bubble appearance)
4. No reactive sclerosis
5. No periosteal reaction in absence of fracture

Giant cell tumour of distal radius

Giant cell tumour of proximal tibia

Multiloculated lesion with a very characteristic appearance (honeycomb-like pattern) (left); Pure lytic lesion (right)
Giant Cell Tumour Link List
- Giant Cell Tumour
- Learn more about Giant Cell Tumour
METASTASIS - RENAL CELL CARCINOMA
Since the kidney is comprised of mostly blood vessels, kidney cancer metastases may also have a rich blood supply, and may bleed extensively (even audibly) after a simple biopsy.
Other lytic but non-expansile metastasis include lung and thyroid cancer.

Renal cell carcinoma metastasis to pelvis
Skeletal Metastasis Link List
- Skeletal Metastasis
- Learn more about skeletal metastasis
- Skeletal Metastasis AAOS
- Skeletal Metastasis at AAOS
Multiple Myeloma
It is the most common primary bone tumour and is found in the spine, skull, ribs, sternum and pelvis.
It is a malignant tumour of plasma cells that causes widespread osteolytic bone damage.
The average patient age is over 50 years old.
Men are affected twice as often as women.
It tends to involve the entire skeleton.
Characteristic X-Ray Finding of Multiple Myeloma
Multiple myeloma appears on X-rays as decreased bone density with a lot of "punched out" holes in the bone.
Erosion begins intramedullarly and progresses through the cortex.
These destructive lesions are not surrounded by the white rim of bone seen in other types of destructive lesion.

Multiple "punched-out" lesion in the skull

Multiple Myeloma of long bones
Plasma Cells
The osteolytic lesions are caused by increased osteoclastic resorption that is stimulated by cytokines released by-the plasma cells.

Plasma cells
Multiple Myeloma Link List
- Multiple Myeloma
- Learn more about multiple myeloma
Aneurysmal Bone Cyst
Hallmark is ballooned-out appearance
Eccentric location
Marked cortical thinning and erosion and periosteal elevation.
Buttress of periosteal reaction (to differentiate from simple bone cyst)
Usual containment by a thin shell of periosteum
Lesion rarely penetrates the articular surface or growth plate.
Radiographic differential diagnosis includes:
1. Simple bone cyst
2. Giant cell tumor of bone
3. Telangiectatic osteosarcoma
4. Angiosarcoma.

Anuerysmal bone cyst of proximal femur
ANEURYSMAL BONE CYST - SPINE

Chondroblastoma
Chondroblastomas are radiolucent lesions that typically occupy the epiphysis (or apophysis) of long bones.
They tend to be small (<>

Plain radiograph of the distal femoral epiphysis in a 12-year-old boy. This image shows a chondroblastoma with a characteristica

Plain radiograph of the greater trochanter in a 24-year-old man. Chondroblastomas that occur in the proximal femur are 3 times m
Hemangioma
Benign lesions characterized by vascular spaces lined with endothelial cells.
50% of osseous hemangiomas are found in the vertebral bodies (thoracic especially) and 20% in the calvarium.
The remaining lesions are found in the tibia, femur and humerus.
The radiological appearance can be quite striking and depends on the location of the lesion.
The lesions are often poorly defined, appearing as a somewhat localized area of abundant, dilated vessels, some of which may be on the surface of the b

Hemangioma of tibia

Hemangioma of vertebra
HEMANGIOMA SPINE
 On CT scan, vertebral body lesions have a "polka dot" pattern as the vessels are seen in cross section.
On CT scan, vertebral body lesions have a "polka dot" pattern as the vessels are seen in cross section.Calvaria lesions are lytic and resemble radiating wheel spokes.
INFECTION (OSTEOMYELITIS)
 IN CHILDREN:
IN CHILDREN:Pathomechanism
1.Trans-physeal vessels closed
2.Primary focus of infection is in metaphysis
Findings
* Sequestration frequent
* Periosteal elevation
* Small single / multiple osteolytic areas in metaphysis
* Extensive periosteal reaction parallel to shaft (after 3-6 weeks)
* Shortening of bone with destruction of epiphyseal cartilage
* Growth stimulation by hyperemia and premature maturation of adjacent epiphysis
NON OSSIFYING FIBROMA
 AKA: Nonosteogenic fibroma, fibroxanthoma, xanthogranuloma of bone.
AKA: Nonosteogenic fibroma, fibroxanthoma, xanthogranuloma of bone.30 to 40% children over two years have one or more lesions.
Most common between 8-20 years of age.
Usually occur in metaphysis of one (75%) or more (25%) of the tubular bones.
Most often occur in lower extremities around knee.
Fewer than 10% occur in upper extremities.
Non-ossifying Fibroma
X Ray Characteristics:
1. Geographic
2. Lytic
3. Multilobulated
4. Metaphyseal
5. Usually intramedullary
6. Eccentric (situated in the periphery of bone)
7. Well-marginated
8. Sclerotic rim
9. Endosteal scalloping

Non-ossifying fibroma of tibia
NON OSSIFYING FIBROMA 3
 Most lesions heal spontaneously by being replaced with normal bone.
Most lesions heal spontaneously by being replaced with normal bone.Migrate away from epiphysis with growth of patient.
May undergo pathologic fracture (picture).
Do not undergo malignant transformation
EOSINOPHILIC GRANULOMA
 Solitary, non-neoplastic proliferation of histiocytes.
Solitary, non-neoplastic proliferation of histiocytes.Part of a spectrum of Langerhan's cell histiocytosis, formerly known as histiocytosis X.
Localized lesion in bone or lung and occurs most commonly in children aged 5 to 10.
The skull may have a lesion with sharp, punched out borders (picture).
ENCHONDROMA
 Benign cartilaginous tumor.
Benign cartilaginous tumor.Develops in the medullary cavity.
Usually solitary (multiple lesions in syndromes).
Arise from ectopic rests of hyaline cartilage.
Occur mostly in 2nd to 3rd decade.
Most common site is small bones of the hands and feet.
Most occur in the proximal phalanx.
Usually asymptomatic and found insidiously.
Rapid growth with pain and swelling should raise suspicion of either a pathologic fracture or, less likely, malignant transformation.
Enchondroma X Ray Finding
X-Ray finding:
Well-defined lytic and slightly expansile lesion (in small bones).
Usually have some internal calcification and endosteal thinning.
Internal calcifications tend to resemble "rings and arcs" of cartilage calcification .

There is an expansile, lucent, well-defined ("geographic") lesion with swirls and rings of chondroid calcification at the

Enchondroma in the distal femur. Note the lesion is geographic with response from surrounding bone. Cartilagenous matrix is pr
Enchondroma Link List
- Enchondroma
- Learn more about enchondroma
Multiple Enchondromatosis (Ollier Disease)
This is nonhereditary disorder which usually presents in childhood.
The affected extremity is shortened (asymmetric dwarfism) and sometimes bowed due to epiphyseal fusion anomalies.
Patients are at risk for development of sarcomas, specifically osteosarcomas and chondrosarcomas. These occur in approximately 25 % of patients.

Multiple enchondromas are present in this radiograph of the left hand in a patient with Ollier disease. Lesions for unknown rea

The left distal femur is widened with an "Erlenmeyer" deformity. The left femur is also shortened relative to the right. The med
New The Most Important Thing
MULTIPLE ENCHONDROMATOSIS (MAFUCCI SYNDROME)
 Nonhereditary
NonhereditaryEven more rare than Ollier's disease
Multiple cavernous hemangiomas of soft tissues, usually in extremities (digits)
Look for phleboliths in hemangioma
The typical appearance of Mafucci syndrome is illustrated by this radiograph.
Multiple enchondromas are encountered along with phleboliths in soft tissue hemangiomas.
MAFUCCI SYNDROME
 Growth disturbance of affected bones
Growth disturbance of affected bonesMalignant transformation common -75%
Hemangioma may become sarcoma in 5% of cases.
Mafucci syndrome
Mafucci syndrome represents enchondromatosis with soft tissue hemangiomas, usually in the hands and feet.
As with Ollier disease, there is typically a shortening of the long bones.
These patients are at higher risk for sarcomatous transformation of both the vascular and cartilaginous portions of the disease.

Multiple enchondromas are encountered along with phleboliths in soft tissue hemangiomas.
MAFUCCI SYNDROME
 Intra operative finding of hemangioma
Intra operative finding of hemangioma SOLITARY BONE CYST
 Pathogenesis - Theories
Pathogenesis - TheoriesFocal defect in metaphyseal remodelling causing blockage in interstitial drainage .
This increases the intraosseous pressure leading to focal bone necrosis and accumulation of fluid .
Fluid causes bony destruction due to presence of prostaglandin, oxygen free radicals, interleukin, cytokines and metalloproteinases .
Prostaglandin - stimulate osteoclasts to resorb bone and subsequently leads to more fluid accumulation.
SOLITARY BONE CYST 3
 Indication for treatment- To reduce the potential risk of pathological fracture and to alleviate pain
Indication for treatment- To reduce the potential risk of pathological fracture and to alleviate painOptions:
- Steroid Injection
- Curretage and bone graft
- Injection of fibrosing agents
- Percutaneous autologus bone marrow injection
- Percutaneous demineralized bone matrix injection
Solitary (Unicameral) Bone Cyst
Purely lytic lesion
Metaphyseal , diaphyseal region
Concentric lesion
Septated
Thin cortex

Solitary bone cyst of proximal humerus with fallen leaf sign signifying pathological fracture
Simple Bone Cyst Link List
- Unicameral Bone Cyst
- Learn more about simple bone cyst
Wise Sayings About Solitary Lucent Lesions
1. With a long lesion in a long bone, think of fibrous dysplasia.
2. Simple cyst, enchondroma, and fibrous dysplasia can mimic each other and can be hard to distinguish. Thus, when you think of one of these three entities, also think of the other two.
3. Giant cell tumors nearly always occur near a joint surface.
4. For lucent lesions in patella, calcaneum, and most apophyses, one should include the classic epiphyseal entities such as chondroblastoma, giant cell tumors and aneurysmal bone cys
New Featured Lenses
-
 SPINE ARTHRITIS
SPINE ARTHRITIS -
The spine is made up of both synovial joints and non-synovial joints. The synovial joints are found in the facet joints, the unco-vertebral joints of cervical spine, the costovertebral joints and the sacroiliac joints. The non-synovial joints a...
-
 SOFT TISSUE CALCIFICATION
SOFT TISSUE CALCIFICATION -
Soft tissue calcifications are usually caused by one of the following 5 entities. These are listed below in order of prevalence. (Note: Do not confuse soft tissue calcification with bone calcification. Bone calcification will be dealt in Bone Tum...
-
 Bone Tumour Radiology
Bone Tumour Radiology -
1. Clues by appearance of lesion 2. Clues by location of lesion 3. Clues by type of periosteal reaction 4. Clues by matrix of lesion 5. Clues by density of lesion 6. Clues by number of lesion
-
 Sclerotic Bone Lesion
Sclerotic Bone Lesion -
Generally bone sclerosis signifies a slow-growing process. Bone reacts to disorder in two ways -- either by removing some of itself or by creating more of itself. If the disorder is rapidly progressive, there may only be time for retreat, hence...
-
 Periosteal Reaction
Periosteal Reaction -
The periosteum is a membrane several cell layers thick that covers almost all of every bone. The only parts not covered by this membrane are the parts covered by cartilage.
New Featured Lenses
-
 Osteosarcoma
Osteosarcoma -
Osteogenic Sarcoma (osteosarcoma) is a bone forming cancer. It is the most frequent type of bone tumour and is most common between the ages of 15 to 25. Over 90% of tumours are located in the metaphysis (the growing ends of the bone), the mos...
-
 Giant Cell Tumour
Giant Cell Tumour -
Giant cell tumour is a benign but locally aggressive tumour with a potential to metastasize.
-
 TOTAL KNEE REPLACEMENT
TOTAL KNEE REPLACEMENT -
Total knee replacement offers the greatest quality of life improvement of all operations. It has one of the highest success rates and one of the best outcomes.
-
 Skeletal Metastasis
Skeletal Metastasis -
Cancer affecting the skeleton is more often metastatic than primary The skeleton is the 3rd most common site for metastases The axial skeleton is involved in 70% of cases...
-
 Limb Salvage Surgery
Limb Salvage Surgery -
Limb salvage surgery is made possible due to advances in: 1. Neoadjuvant and adjuvant chemotherapy 2. Good diagnostic imaging (CT Scan, MRI) 3. Advanced surgical techniques

No comments:
Post a Comment