How to read elbow x-ray at a glance
By Dr. KM Liau

Fractures lines can be difficult to visualize after acute elbow injury, particularly in children.
Below are 7 essential steps to help you.
Step 1- Hourglass Sign
Search for an adequate "hourglass sign", or "figure of eight" at the distal humerus.
Here's an example of a true lateral; note the symmetric figure of eight/hourglass sign at the distal humerus

If absent the study is not a true lateral and interpretation of steps 2 through 4 is less reliable.
Here's an example of a true lateral; note the symmetric figure of eight/hourglass sign at the distal humerus
If absent the study is not a true lateral and interpretation of steps 2 through 4 is less reliable.
Asymmetric Hourglass
Here is an imperfect lateral radiograph.
Notice how the figure of eight/hourglass is asymmetric.

Notice how the figure of eight/hourglass is asymmetric.
Step 2 - Abnormal anterior fat pad
An abnormal anterior fat pad is described as a "sail sign" because it is unusually prominent and bows outward to form a triangular shape.
After trauma, blood can accumulate in the intraarticular space and push the fat pad anteriorly; a positive sail sign in the setting of trauma is a reliable indication of an intraarticular fracture - even if no fracture line can be identified.
An atraumatic sail sign implies intraarticular fluid of an inflammatory nature.
Radiographic visualization of a posterior fat pad is never normal and always signifies fluid in the intraarticular space. Again, in the setting of trauma, this strongly implies fracture of an articular surface.
Here is a radiograph with both a sail and posterior fat pad sign:

After trauma, blood can accumulate in the intraarticular space and push the fat pad anteriorly; a positive sail sign in the setting of trauma is a reliable indication of an intraarticular fracture - even if no fracture line can be identified.
An atraumatic sail sign implies intraarticular fluid of an inflammatory nature.
Radiographic visualization of a posterior fat pad is never normal and always signifies fluid in the intraarticular space. Again, in the setting of trauma, this strongly implies fracture of an articular surface.
Here is a radiograph with both a sail and posterior fat pad sign:
Step 3 - Anterior Humeral Line
The yellow line represents the anterior humeral line and the red line represents the proximal radial line.
The important observation regarding these lines is that they should intersect the middle third of the capitellum on the lateral view.
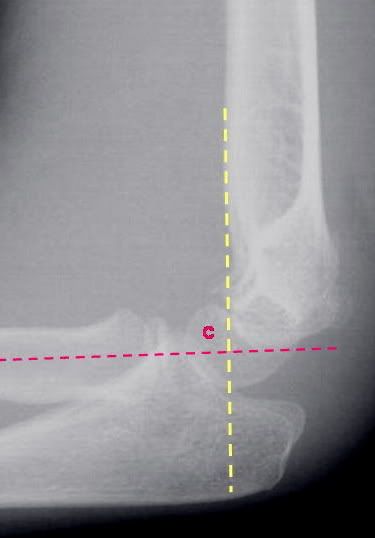
Fractures usually result in displacement of the capitellum posteriorly.
If the film is not a true lateral, interpretation of the anterior humeral line becomes fallible.
The important observation regarding these lines is that they should intersect the middle third of the capitellum on the lateral view.
Fractures usually result in displacement of the capitellum posteriorly.
If the film is not a true lateral, interpretation of the anterior humeral line becomes fallible.
Abnormal Anterior Humeral Line
This radiograph demonstrates abnormal alignment of the anterior humeral line strongly suspicious for fracture.
The anterior humeral line of a toddler/child must also intersect the middle third of an ossified capitellum.
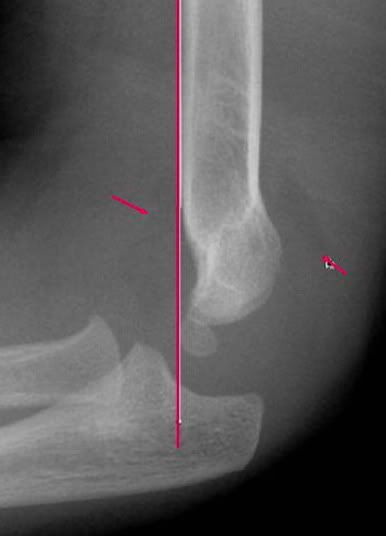
Also note the posterior fat pad and sail sign.
The anterior humeral line of a toddler/child must also intersect the middle third of an ossified capitellum.
Also note the posterior fat pad and sail sign.
Step 4 - Radio-capitellar line
This line is drawn through the middle of the radius and should bisect the capitellum on both the lateral and the AP elbow radiograph.
Failure to align properly indicates a radial head dislocation that requires prompt reduction if neuro-vascular compromise is to be avoided.
Failure to align properly indicates a radial head dislocation that requires prompt reduction if neuro-vascular compromise is to be avoided.
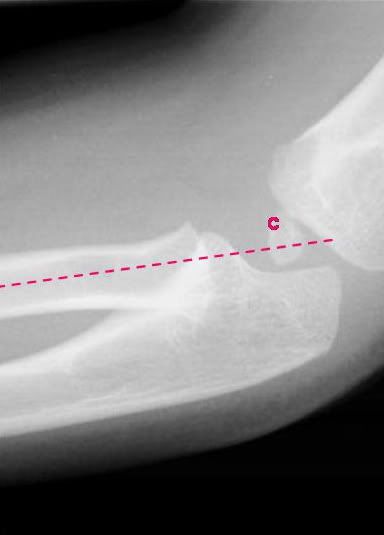
AP view of Radio-capitellar line
Note that the line passes through the center of capitellum.

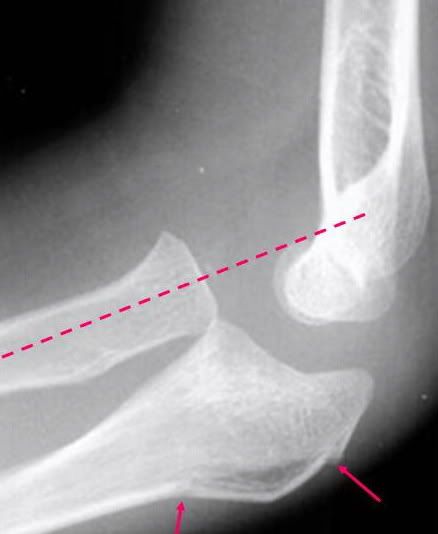
Abnormal Radio-capitellar line
On AP view the radius fails to bisect the capitellum indicating an obvious radial head dislocation.

Abnormal Radio-capitellar line
Also note the anterior and posterior fat pads, as well as the obvious olecranon deformity.
A radial head dislocation with an olecranon fracture is called a Monteggia injury.
A radial head dislocation with an olecranon fracture is called a Monteggia injury.
Step 5 - Inspection of the radial head
Notice how the radius bisects the capitellum on this view.
However there is a subtle cortical disruption/acute angulation at the superior aspect of the distal radius indicating fracture.

However there is a subtle cortical disruption/acute angulation at the superior aspect of the distal radius indicating fracture.
Step 6 - Distal Humerus Examination
Signs of humeral fracture are also commonly subtle; breakage may only be evidenced by an abnormal anterior humeral line.
Exam this radiograph.

Exam this radiograph.
Abnormal Anterior Humeral Line
The anterior humeral line is perhaps slightly off as it seems to intersect the anterior third of the capitellum, while the radio-capitellar line is intact.

There are prominent sail and posterior fat pad signs; and on careful inspection one sees the subtle cortical disruption along the posterior aspect of the distal humerus.
There are prominent sail and posterior fat pad signs; and on careful inspection one sees the subtle cortical disruption along the posterior aspect of the distal humerus.
Step 7 - Olecranon and Ulnar Examination
Look for obvious fracture lines and subtle disruptions in cortical contour.

This is not a good lateral radiograph so interpretation of the anterior humeral line is unreliable. There is no obvious anterior or posterior fat pad, and the radio-capitellar line is intact. The radial head and distal humerus appear fine, while there is an obvious proximal olecranon fracture.
This is not a good lateral radiograph so interpretation of the anterior humeral line is unreliable. There is no obvious anterior or posterior fat pad, and the radio-capitellar line is intact. The radial head and distal humerus appear fine, while there is an obvious proximal olecranon fracture.
The Most Important Thing
1. Know where is the capitellum - the center point of elbow.
2. Find the intersection line.
3. Look for fat pad sign.
Statistics
The frequency of elbow dislocations is second to that of dislocations of the shoulder.
Posterior dislocations of the elbow are the predominant type and account for 80-90% of all elbow dislocations.
About 30% of elbow fractures in adults occur in the radial head.
Olecranon process fractures account for 20% of all elbow injuries in adults.
Coronoid process fractures occur in 10-15% of dislocations of the elbow.

very good article......thanks doctor ....continue such efforts..........................dr radhey shyam,New Delhi,India
ReplyDeletei like this article very much.the radiographs are also very clear.hope to see more articles from you.
ReplyDelete...............PG ASPIRANT.