Ankle and Foot X Ray

Fractures of the foot and ankle are common injuries. This lens will take you through the common foot and ankle fractures.
Functional Anatomy
Stability of the ankle mortise relies on the configuration of the osseus structures and the ligaments.
The main articulation is between the talus and the tibial plafond.
The saddle-shaped dome of the talus fits exactly into the tibial plafond and small disturbances in the congruity of this tibiotalar joint reduce the contact area and will overload the articular cartilage leading to arthrosis.
The Syndesmosis Ligament

Normal Ankle X Ray
On a true AP-view the talus overlaps a portion of the lateral malleolus obscuring the lateral aspect of the ankle joint (left image).
AP-view will give you a extra view on both malleoli from a different angle.

The Mortise-view (right picture) is an AP-view with 15-25° internal rotation of the foot.
The technologist turns the foot inwards until the lateral malleolus is at the same height as the medial malleolus.
This view clearly demonstrates both lateral and medial joint spaces.
Ottawa Ankle Rules
Ankle X-ray series is required only if there is
pain in the malleolar zone and any one of the following:
1. Bone tenderness along the distal 6 cm of the posterior edge of the fibula or tip of the lateral malleolus.
2. Bone tenderness along the distal 6 cm of the posterior edge of the tibia or tip of the medial malleolus.
3. Inability to bear weight for 4 steps both immediately and in the emergency department.

Malleolar zone in white. Distal pole of tibia and fibula in blue.
Fracture mechanism

LEFT. The medial malleolus is pulled off by the medial collateral ligament as in pronation (eversion) trauma.
RIGHT. The medial malleolus is pushed off as in supination (inversion) trauma
Stable or Unstable
The ankle can be considered as a ring in which bones as well as ligaments play an equally important role in the maintenance of the stability of the joint.
If the ring is broken in one position the ring remains stable.
When it is broken in two positions the ring is unstable because a portion of it can be or is dislocated.
Medial and Lateral Clear Space in Mortise View
Widening of the ankle mortise is another sign of ligamentous rupture.
The medial clear space should not exceed 4 mm and usually measures the same as the distance between the tibial plafond and the talus.
Widening of the medial joint space up to 6 mm or more requires disruption of the medial collateral ligament.
The lateral clear space is measured from the medial border of the fibula to the lateral border of the posterior tibia 1cm above the tibial plafond.
It is less well defined because it's width varies with positioning.
Evident widening of the lateral clear space indicates syndesmotic rupture.
Some however state that a width of 5.5mm is abnormal.
Normal Clear Space Does Not Exclude Ankle Instability
A normal lateral or medial clear space however does not exclude ligamentous rupture.
It simply means that there is no dislocation, but there still can be instability.
Weber Classification of Ankle Fracture
The higher the level the more chance for syndesmotic rupture and instability.
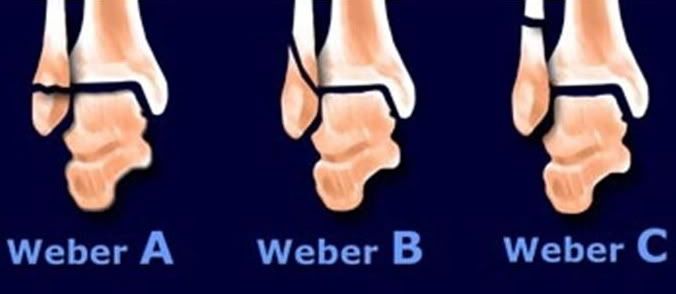
Weber A Fracture

Basic interpretation: Transverse lateral malleolar fracture.
Classification: Weber A
Treatment - Patient will be treated conservatively in view of the stable fracture.
Weber B Fracture

The left image shows a Weber B fracture.
Both medial and lateral clear space are widened indicating instability.
The talus is displaced laterally.
Patient was sceduled for osteosynthesis of the fibula fracture and placement of a syndesmotic screw if necessary.
After osteosynthesis of the fibula, the ankle was tested in the operating room and found to be stable.
So there was no indication for placement of a syndesmotic screw.
So we can conclude that the syndesmosis was only partially ruptured (as is usually the case in Weber B fractures).
Weber B - Inadequate Fixation

LEFT: After osteosynthesis there is widening of medial and lateral clear space.
RIGHT: Patient was re-operated and a syndesmotic screw was inserted to restore tibiotalar alignment.
Weber B - Trimalleolar Fracture

Basic interpretation: dislocated bimalleolar fracture.
Avulsion of the medial malleolar fracture.
The lateral malleolus is 'pushed off' from anterior to posterior.
The fracture starts at the level of the ankle joint and extends proximally.
Classification: Weber type B fracture.
Re-examination: Look for posterior syndesmotic rupture or avulsion of the posterior malleolus and rupture of the deltoid ligament or medial malleolar avulsion).
Only now you notice the posterior malleolar fracture on the lateral view.
Final report: Trimalleolar fracture. Weber B.
This is an unstable fracture with dislocation that needs surgical repair.
The size of the posterior malleolar fragment is probably less than 25% of the articular AP-diameter and will need no separate repair.
Sometimes CT is needed to get a better impression of the size of the fracture fragment of the posterior malleolus.
Weber C - Bimalleolar Fracture

Basic interpretation: displaced bimalleolar fracture.
Avulsion fracture of the medial malleolus %uFF08pulled off%uFF09.
The lateral malleolus is fractured more than 5 cm from the ankle joint line%u3002
Opening up of the syndesmotic joint
Increased medial clear space
Talus is externally rotated
Classification: Weber type C fracture.
Treatment - This is an unstable fracture which requires internal fixation
Talar body fracture
AP View

This is displaced intrarticular fractures requiring internal fixation..
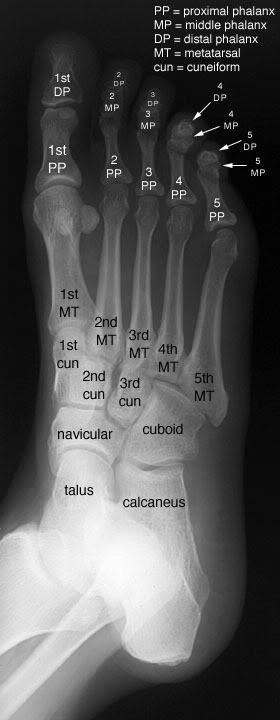
Foot AP View
The medial margin of the base of the second metatarsal should be inh line with the medial margin of the middle cuneiform in this view.

Foot - Oblique View.
The medial margin of the base of the third metatarsal should be in line with the medial margin of the lateral cuneiform in this view.
Metatarsal Fracture

Jones' Fracture
 A Jones' fracture is a fracture of the base of the fifth metatarsal of the foot.
A Jones' fracture is a fracture of the base of the fifth metatarsal of the foot.It was named after Sir Robert Jones, who in 1902, sustained this fracture while dancing around a maypole at a garden dance.
The injury is caused by stress plantarflexion and inversion.
Jones' Fracture

1. This location is an area of poor blood supply. In medical terms it is a watershed area between two blood supplies.
2. In addition there are various tendons attaching in the area pulling the fracture apart causing motion at the site of healing.
Jones Fracture
This fracture is optimally treated with screw fixation to provide compression of the fracture which enhances union rate.

No comments:
Post a Comment